
Primitive Reflexes: The Earliest Language of the Nervous System
Exploring the earliest movement programs that guide human neurological development

By Dr. David Traster, DC, MS, DACNB
Co-owner, The Neurologic Wellness Institute
Boca Raton • Chicago • Waukesha • Wood Dale
www.neurologicwellnessinstitute.com
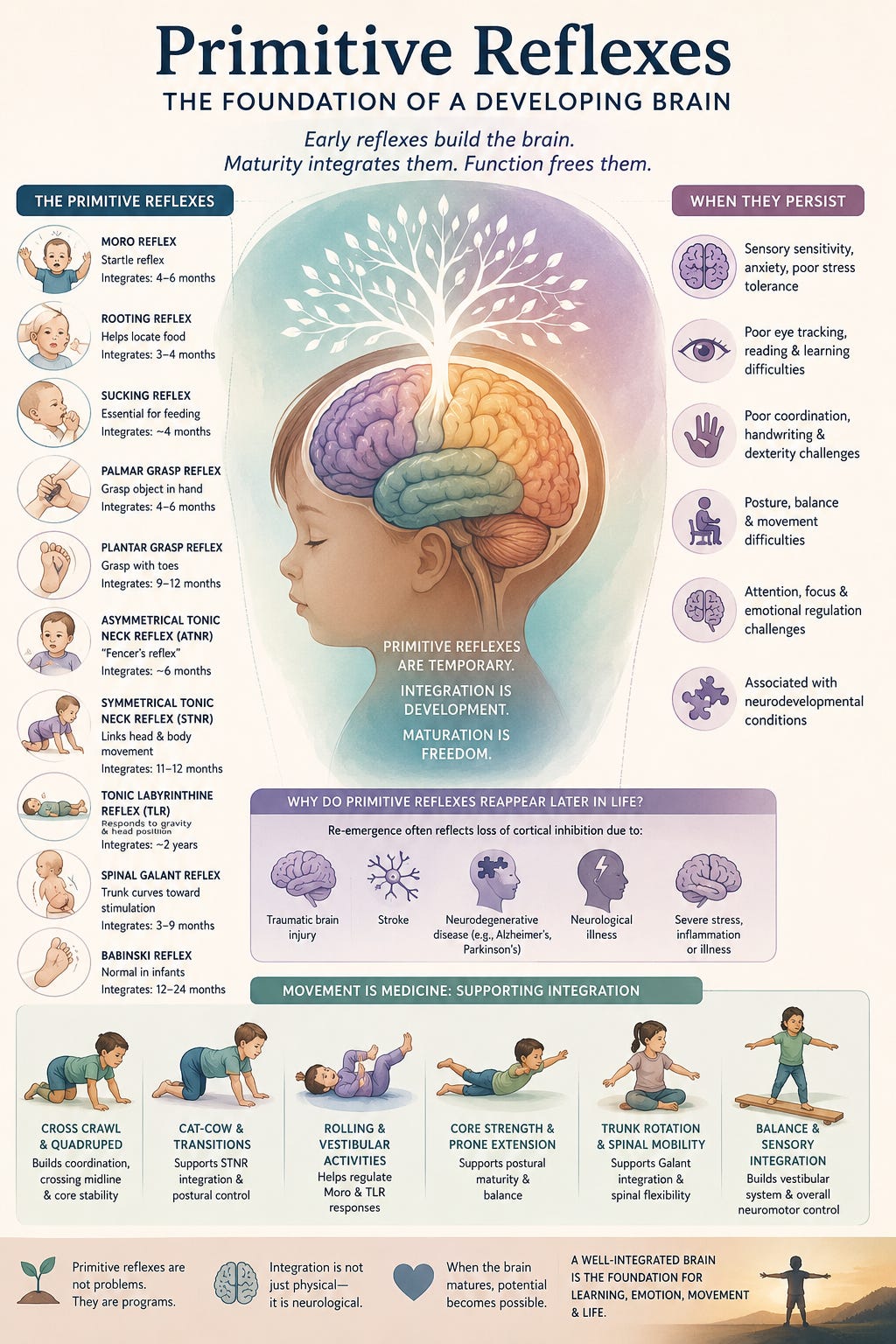
Before a child can sit, crawl, walk, speak, or consciously interact with the world, the nervous system communicates through a series of automatic movement patterns known as primitive reflexes. These reflexes are among the earliest signs of neurological function and represent the foundational building blocks upon which higher levels of motor control, cognition, posture, sensory integration, and emotional regulation are constructed. Primitive reflexes emerge during fetal development and infancy and are designed to help the newborn survive, interact with the environment, and stimulate maturation of the developing brain. As the nervous system matures, these reflexes should gradually become inhibited or integrated by higher brain centers. Their disappearance is not a loss of function but rather a sign that more advanced neural networks have taken control.
Why Primitive Reflexes Exist
Primitive reflexes serve several critical purposes during infancy. They assist with birth, feeding, protection, sensory exploration, muscle tone development, postural control, and the establishment of early movement patterns. They create sensory feedback loops that stimulate the development of the brainstem, cerebellum, basal ganglia, and cerebral cortex. Every time an infant moves through a primitive reflex pattern, information travels throughout the nervous system, helping to organize neural connections that will eventually support voluntary movement and higher cognitive functions.
In many ways, primitive reflexes act like developmental scaffolding. Just as scaffolding supports a building during construction and is removed once the structure is complete, primitive reflexes support neurological development until higher cortical systems become sufficiently mature to assume control.
The Moro Reflex
The Moro reflex, often called the startle reflex, emerges around 28–32 weeks gestation and is fully present at birth. It is triggered by sudden head movement, loud sounds, bright lights, or unexpected sensory stimuli. The infant responds by extending the arms and legs outward, opening the hands, and then rapidly bringing the limbs back toward the body.
This reflex is primarily generated within the brainstem, particularly the vestibular nuclei and reticular formation. It typically integrates between four and six months of age.
The Moro reflex helps prepare the infant to respond to perceived threats and stimulates activation of the autonomic nervous system. Persistence beyond infancy has been associated with hypersensitivity to sensory stimuli, anxiety, emotional dysregulation, poor stress tolerance, attention difficulties, and autonomic dysfunction.
The Rooting Reflex
The rooting reflex appears around 28 weeks gestation and assists infants in locating a food source. Stroking the cheek causes the infant to turn toward the stimulus and open the mouth.
This reflex is mediated through cranial nerve pathways involving the trigeminal and facial nerves and is coordinated within the brainstem. It typically disappears between three and four months of age.
Persistence may contribute to oral fixation behaviors, speech difficulties, feeding challenges, and poor oral motor coordination.
The Sucking Reflex
The sucking reflex develops during fetal life and is critical for feeding and survival. Stimulation of the lips or palate automatically initiates rhythmic sucking movements.
Brainstem pattern generators involving cranial nerves V, VII, IX, X, and XII coordinate this reflex. It generally becomes voluntary by four months of age.
Retention may contribute to speech articulation problems, tongue thrusting, swallowing abnormalities, and difficulties with oral motor control.
The Palmar Grasp Reflex
The palmar grasp reflex is present at birth and causes the infant to tightly grasp an object placed in the palm.
This reflex is mediated through spinal cord circuits and brainstem pathways. It usually integrates between four and six months.
Persistent palmar grasp reflexes may be associated with poor handwriting, immature fine motor skills, hand fatigue, difficulty with dexterity, and impaired hand-eye coordination.
The Plantar Grasp Reflex
Pressure applied to the sole of the foot causes toe flexion and gripping.
This reflex originates within spinal cord and brainstem pathways and generally integrates by 9 to 12 months.
Persistence may interfere with balance development, gait mechanics, toe walking, and postural stability.
The Asymmetrical Tonic Neck Reflex (ATNR)
The ATNR is often called the “fencer’s reflex.” Turning the infant’s head to one side causes extension of the arm and leg on the face side and flexion on the skull side.
This reflex emerges around 18 weeks gestation and integrates by six months of age. It is primarily coordinated by vestibular and cervical proprioceptive pathways within the brainstem.
The ATNR helps establish hand-eye coordination, visual tracking, and awareness of body sides. Persistent ATNR has been associated with difficulties crossing midline, reading problems, poor handwriting, visual tracking deficits, and challenges with bilateral coordination.
The Symmetrical Tonic Neck Reflex (STNR)
The STNR emerges later, usually between six and nine months, and should integrate by 11 to 12 months.
Flexing the neck causes arm flexion and leg extension, while neck extension causes arm extension and leg flexion.
The STNR serves as a bridge between primitive reflexes and mature postural control and is critical for crawling development.
Retention may contribute to poor posture, slouching, difficulty sitting still, visual problems, and impaired motor coordination.
The Tonic Labyrinthine Reflex (TLR)
The TLR is heavily influenced by vestibular input. Head position relative to gravity influences muscle tone throughout the body.
In prone positions, flexor tone dominates. In supine positions, extensor tone dominates.
The vestibular nuclei, cerebellum, and reticular formation play major roles in generating this reflex. It normally integrates by approximately two years of age.
Persistence may result in balance deficits, poor posture, motion sensitivity, visual dysfunction, spatial disorientation, and coordination problems.
The Spinal Galant Reflex
Stroking one side of an infant’s back causes lateral trunk flexion toward the stimulus.
This reflex is mediated through spinal cord pathways and is normally integrated between three and nine months.
Retention has been associated with fidgeting, poor sitting posture, bedwetting, scoliosis tendencies, attention difficulties, and sensory hypersensitivity around the waist.
The Babinski Reflex
Stroking the sole of the foot causes extension of the great toe and fanning of the remaining toes.
Babinski is normal in infants because the corticospinal tract is not yet fully myelinated. It typically disappears by 12 to 24 months.
The presence of a Babinski sign in adults usually indicates corticospinal tract dysfunction and is one of the classic signs of upper motor neuron pathology.
What Does It Mean When Primitive Reflexes Persist?
The persistence of primitive reflexes beyond their expected developmental window suggests incomplete maturation or insufficient inhibition from higher brain centers. In healthy neurological development, cortical networks, basal ganglia circuits, cerebellar systems, and descending motor pathways gradually suppress primitive reflex activity.
Retained reflexes do not necessarily indicate structural brain damage. However, they may reflect developmental delays, sensory integration dysfunction, neurodevelopmental disorders, traumatic brain injury, chronic neurological stress, vestibular dysfunction, or impaired connectivity within cortical-subcortical networks.
Research has demonstrated increased rates of retained primitive reflexes in conditions such as ADHD, autism spectrum disorders, learning disabilities, developmental coordination disorder, traumatic brain injury, and various movement disorders.
Why Primitive Reflexes Reappear Later in Life
Primitive reflexes may re-emerge when previously mature neural systems become damaged or dysfunctional.
This phenomenon is often referred to as “frontal release” because many primitive reflexes are normally suppressed by frontal lobe and cortical inhibitory networks. When these systems deteriorate, older neurological programs become unmasked.
Primitive reflex re-emergence is commonly seen in dementia, Alzheimer’s disease, Parkinson’s disease, frontal lobe disorders, stroke, traumatic brain injury, hydrocephalus, multiple sclerosis, severe encephalopathy, and other neurodegenerative conditions.
The reappearance of primitive reflexes reflects a loss of top-down cortical control and often serves as an important neurological examination finding.
Primitive Reflexes and Brain Maturation
Primitive reflex integration is essentially a visible marker of nervous system development. As infants mature, control gradually shifts from lower brainstem and spinal circuits toward cerebellar, basal ganglia, thalamic, and cortical networks.
The disappearance of primitive reflexes therefore represents increasing neurological sophistication. The nervous system moves from automatic survival-based responses toward adaptable, voluntary, and goal-directed behavior.
For clinicians, primitive reflex testing offers a unique window into developmental neurophysiology and can provide valuable information regarding nervous system maturity and integrity throughout the lifespan.
Exercises Used to Remediate Retained Primitive Reflexes
Numerous developmental and rehabilitation programs utilize exercises designed to replicate normal infant movement patterns. The goal is to provide repetitive sensory and motor experiences that encourage integration of retained reflexes and strengthen higher neural networks.
For retained ATNR, activities often include crawling patterns, cross-crawl exercises, quadruped movements, contralateral reaching tasks, and coordinated eye-head movements.
For retained STNR, cat-camel exercises, crawling drills, quadruped rocking, and transitional posture exercises are commonly used.
For retained Moro reflexes, vestibular rehabilitation, controlled rolling movements, rhythmic rocking, diaphragmatic breathing, balance training, and autonomic regulation exercises are frequently employed.
For TLR retention, rolling patterns, vestibular stimulation, prone extension activities, balance training, and postural exercises are commonly prescribed.
For spinal Galant retention, trunk rotation exercises, crawling activities, spinal mobility drills, and sensory integration techniques are often utilized.
Modern rehabilitation approaches frequently combine developmental movement patterns with vestibular therapy, cerebellar rehabilitation, visual training, sensory integration, balance exercises, neuroplasticity-based interventions, and functional neurological rehabilitation.
Final Thoughts
Primitive reflexes represent some of the oldest and most fundamental programs within the human nervous system. They guide survival during infancy, stimulate neurological development, and help organize the brain for increasingly complex functions. Their disappearance is a sign of successful maturation, while their persistence or re-emergence can provide valuable clues about neurological development and dysfunction. Understanding primitive reflexes offers a unique perspective into how the brain develops, adapts, compensates, and sometimes regresses. For clinicians, they remain one of the most fascinating examples of how simple reflexive behaviors can reveal profound insights into the organization and health of the nervous system.
References
Blythe, S. G. (2005). The well balanced child: Movement and early learning. Hawthorn Press.
Blythe, S. G. (2017). Neuromotor immaturity in children and adults: The INPP screening test for clinicians and health practitioners. Wiley-Blackwell.
Capute, A. J., Accardo, P. J., Vining, E. P., Rubenstein, J. E., Harryman, S., & Ross, A. (1978). Primitive reflex profile. Developmental Medicine & Child Neurology, 20(5), 571–578.
Futagi, Y., Toribe, Y., & Suzuki, Y. (2012). The grasp reflex and Moro reflex in infants: Hierarchy of primitive reflex responses. International Journal of Pediatrics, 2012, 1–10.
Goddard Blythe, S. (2009). Attention, balance and coordination: The A.B.C. of learning success. Wiley-Blackwell.
Konicarova, J., & Bob, P. (2013). Retained primitive reflexes and ADHD in children. Activitas Nervosa Superior Rediviva, 55(3–4), 135–138.
McPhillips, M., Hepper, P. G., & Mulhern, G. (2000). Effects of replicating primary-reflex movements on reading difficulties in children. The Lancet, 355(9203), 537–541.
Schott, J. M., & Rossor, M. N. (2003). The grasp and other primitive reflexes. Journal of Neurology, Neurosurgery & Psychiatry, 74(5), 558–560.
Zafeiriou, D. I. (2004). Primitive reflexes and postural reactions in the neurodevelopmental examination. Pediatric Neurology, 31(1), 1–8.
Zemke, R., & Clark, F. (1996). Occupational science: The evolving discipline. F.A. Davis Company. (Includes discussion of primitive reflex integration and motor development.)