
Rewiring Depression: How Neuronavigation TMS Is Changing the Timeline of Brain Healing
How Neuronavigation TMS Is Accelerating Brain Healing from Months to Days

By Dr. David Traster, DC, MS, DACNB
Co-owner, The Neurologic Wellness Institute
Boca Raton • Chicago • Waukesha • Wood Dale
www.neurologicwellnessinstitute.com
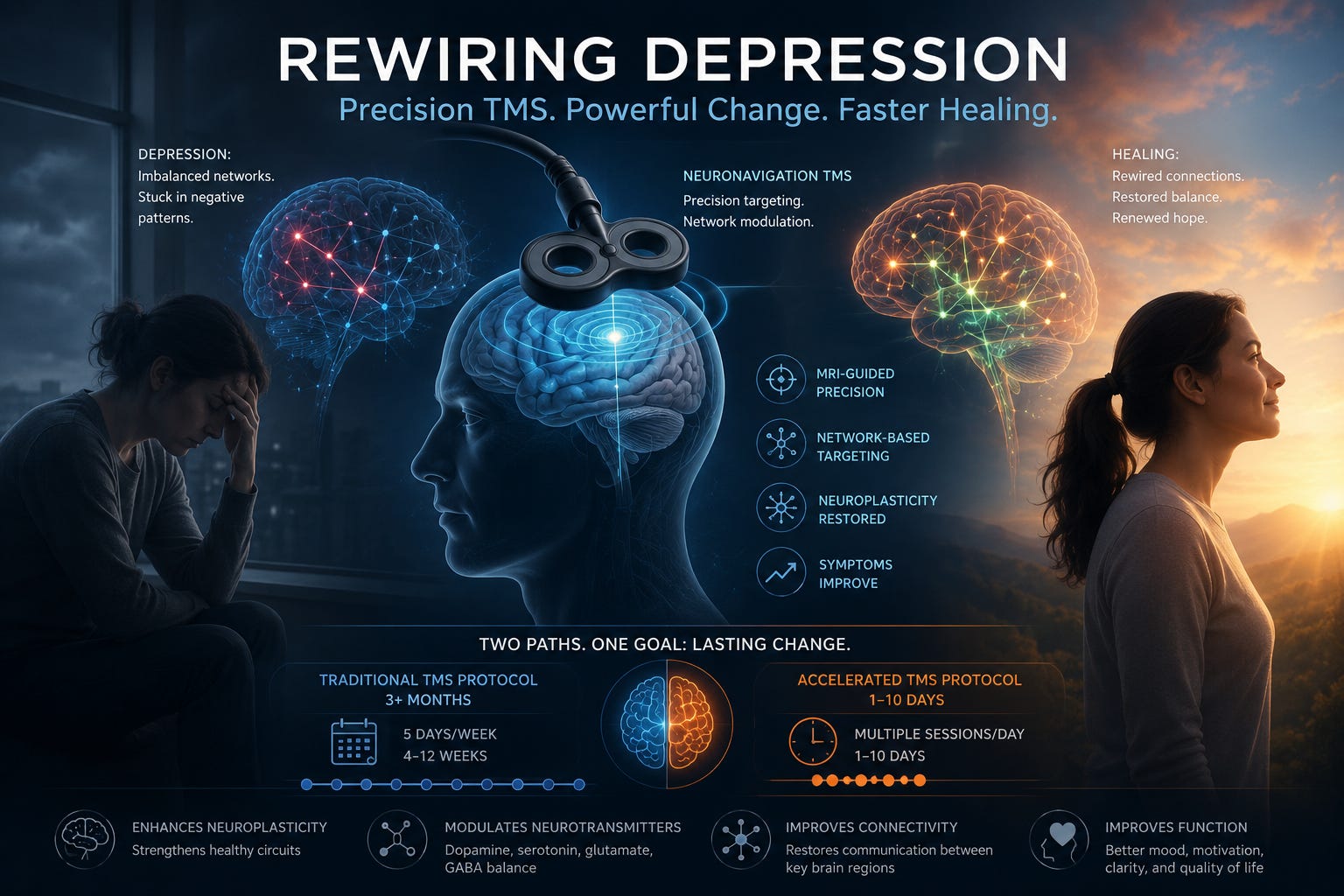
Depression has long been treated as something that improves slowly—weeks to months of medication trials, therapy, and incremental change. But what if the brain could be nudged, guided, and retrained more directly? What if we could target the circuits involved in depression with precision and accelerate recovery—not over months, but potentially in days?
This is the promise of neuronavigation-guided transcranial magnetic stimulation (TMS) and the emergence of accelerated treatment protocols.
The Brain in Depression: A Network Problem, Not a Chemical Imbalance
For decades, depression was framed primarily as a chemical imbalance. While neurotransmitters matter, modern neuroscience has shifted toward a more nuanced understanding: depression is a disorder of brain networks.
Key regions involved include:
The prefrontal cortex (especially the left dorsolateral prefrontal cortex, or DLPFC), responsible for motivation, planning, and cognitive control
The limbic system (including the amygdala), which processes emotion and threat
The default mode network, involved in self-referential thinking and rumination
In depression, these systems become dysregulated:
The prefrontal cortex becomes underactive
Limbic regions become overactive
Network connectivity becomes inefficient and rigid
The result is a brain that becomes “stuck”—locked into patterns of negative thinking, low motivation, and emotional dysregulation.
What Is TMS—and How Does It Work?
Transcranial magnetic stimulation (TMS) is a non-invasive brain stimulation technique that uses focused magnetic pulses to modulate neural activity.
A coil placed on the scalp generates a magnetic field that penetrates the skull and induces electrical currents in targeted brain regions. These currents can:
Increase or decrease neuronal firing
Modify synaptic strength
Influence network connectivity
Unlike medications, which affect the entire brain, TMS is region-specific and circuit-based.
The Power of Neuronavigation: Precision Matters
Traditional TMS often relies on generalized scalp measurements to locate the target region. But no two brains are exactly alike.
Neuronavigation changes that.
Using MRI-guided mapping, clinicians can identify the exact location of a patient’s:
Dorsolateral prefrontal cortex
Functional connectivity patterns
Network imbalances
This allows stimulation to be delivered with millimeter-level precision.
Even more importantly, newer approaches target not just anatomy—but connectivity. For example, identifying the area of the prefrontal cortex most strongly anti-correlated with the subgenual cingulate (a key depression hub) may improve outcomes.
In other words, we are no longer just stimulating the brain—we are tuning its networks.
Traditional TMS: The 6–12 Week Model
Historically, TMS has been delivered over:
4–6 weeks (sometimes up to 12 weeks)
5 sessions per week
Each session lasting about 20–40 minutes
This approach has been effective for many patients, particularly those with treatment-resistant depression. However, it requires a significant time commitment, and improvement can be gradual.
Accelerated TMS: Compressing Time, Amplifying Plasticity
In recent years, a new paradigm has emerged: accelerated TMS protocols.
Instead of spreading sessions out over months, these protocols deliver:
Multiple sessions per day (often 5–10)
Over 1–10 days total
One of the most well-known models is the Stanford Accelerated Intelligent Neuromodulation Therapy (SAINT) protocol, which demonstrated rapid and significant improvements in depression symptoms in some patients.
So what’s different?
1. Intensity and Frequency
By delivering repeated stimulation sessions in a short time window, accelerated TMS may more effectively drive neuroplastic changes—similar to intensive learning.
2. Spaced Learning Principles
Interestingly, sessions are often spaced throughout the day (e.g., hourly), aligning with principles of synaptic potentiation and memory consolidation.
3. Network Reinforcement
Frequent stimulation may reinforce desired network activity before the brain “resets” back to maladaptive patterns.
The Neuroplasticity Behind TMS
At its core, TMS is a tool for inducing neuroplasticity—the brain’s ability to change, adapt, and rewire.
Here’s what’s happening under the surface:
Long-Term Potentiation (LTP) and Depression (LTD)
Repetitive magnetic stimulation can strengthen (LTP) or weaken (LTD) synaptic connections depending on frequency and pattern.
High-frequency stimulation → typically excitatory
Low-frequency stimulation → typically inhibitory
This allows clinicians to:
Upregulate underactive regions (like the left prefrontal cortex)
Downregulate overactive regions (like the right prefrontal cortex or limbic circuits)
Neurotransmitter Modulation
TMS has been shown to influence:
Dopamine (motivation and reward)
Serotonin (mood regulation)
Glutamate (plasticity and excitability)
GABA (inhibition and stability)
Rather than flooding the brain globally, TMS shifts these systems locally and within networks.
Network Reorganization
Perhaps most importantly, TMS helps restore communication between brain regions.
Improves prefrontal-limbic regulation
Reduces hyperconnectivity in rumination networks
Enhances cognitive control over emotional processing
This is not just symptom suppression—it is functional rewiring.
State-Dependent Plasticity
The brain’s response to TMS depends on its current state.
This opens the door to combining TMS with:
Cognitive tasks
Eye movement therapy
Emotional processing
Behavioral activation
In other words, pairing stimulation with meaningful input may enhance outcomes.
Why Faster Might Be Better
Accelerated TMS challenges a long-standing assumption: that brain change must be slow.
In reality, the brain is capable of rapid reorganization under the right conditions.
Consider:
Stroke recovery with intensive rehab
Skill acquisition with focused repetition
Psychedelic-assisted therapy altering networks in hours
Accelerated TMS may tap into similar principles:
High-frequency input
Repetition
Focused targeting
Network-level engagement
For some patients, this can lead to noticeable improvements within days.
Clinical Implications: A Shift in How We Treat Depression
Neuronavigation-guided, accelerated TMS represents a shift from:
Passive treatment → Active brain modulation
Generalized medication → Targeted circuit therapy
Slow timelines → Potentially rapid change
This has major implications for:
Treatment-resistant depression
Acute suicidal ideation
Patients who have failed multiple medications
Individuals seeking non-pharmaceutical options
The Future: Personalized Brain-Based Medicine
We are moving toward a model where treatment is tailored to the individual brain:
MRI-guided targeting
Connectivity-based stimulation
Biomarker-driven protocols
Integration with cognitive and behavioral therapies
TMS is not just a tool—it is a window into how the brain heals.
Final Thoughts: The Brain That Can Change Faster Than We Think
Depression can feel like being trapped in a brain that no longer responds, no longer adapts, no longer shifts.
But that is not the full story.
The brain is plastic. Dynamic. Trainable.
With tools like neuronavigation-guided TMS—especially when delivered in intelligent, accelerated ways—we are beginning to understand that change does not always have to be slow.
Sometimes, under the right conditions, the brain can begin to rewire itself far more quickly than we ever imagined.
And for patients who have been waiting months—or years—for relief, that possibility changes everything.
References
George MS, Lisanby SH, Avery D, et al. Daily left prefrontal transcranial magnetic stimulation therapy for major depressive disorder. Arch Gen Psychiatry. 2010;67(5):507–516.
O’Reardon JP, Solvason HB, Janicak PG, et al. Efficacy and safety of transcranial magnetic stimulation in the acute treatment of major depression. Biol Psychiatry. 2007;62(11):1208–1216.
Fox MD, Buckner RL, White MP, et al. Efficacy of transcranial magnetic stimulation targets for depression is related to intrinsic functional connectivity with the subgenual cingulate. Biol Psychiatry. 2012;72(7):595–603.
Cash RFH, Zalesky A, Thomson RH, et al. Subgenual functional connectivity predicts antidepressant treatment response to transcranial magnetic stimulation. Biol Psychiatry. 2019;85(4):279–286.
Cole EJ, Stimpson KH, Bentzley BS, et al. Stanford Accelerated Intelligent Neuromodulation Therapy for treatment-resistant depression. Am J Psychiatry. 2020;177(8):716–726.
Huang YZ, Edwards MJ, Rounis E, et al. Theta burst stimulation of the human motor cortex. Neuron. 2005;45(2):201–206.
Lefaucheur JP, Aleman A, Baeken C, et al. Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation. Clin Neurophysiol. 2020;131(2):474–528.
Fitzgerald PB, Fountain S, Daskalakis ZJ. A comprehensive review of the effects of rTMS on motor cortical excitability and inhibition. Clin Neurophysiol. 2006;117(12):2584–2596.
Dayan E, Censor N, Buch ER, et al. Noninvasive brain stimulation: From physiology to network dynamics and back. Nat Neurosci. 2013;16(7):838–844.
Liston C, Chen AC, Zebley BD, et al. Default mode network mechanisms of transcranial magnetic stimulation in depression. Biol Psychiatry. 2014;76(7):517–526.
After a year of debilitating depression, major depressive disorder I gave it a try as a last ditch effort. Every day for 6 weeks and I am happy to report it worked amazingly well as well as sustaining post 3 yrs as of today! I am happy to report I am happier than I’ve ever been and feel healthier than ever. I was a sceptic but it proved me wrong.💃
This is so encouraging. Depression is extremely debilitating, and it's worse yet that it can be a silent struggle. I just finished writing an article on this. This disease profoundly disrupts the victim's perception of reality. We are just learning that the brain in all its complexity is capable of healing itself to a certain degree, because as you mentioned it is trainable! Learning other parts of the brain and how it connects, environmental changes, and gently restoring the brain's natural capacity to process data through low-stake inputs could be the first steps to be able to feel, or feel better.