
Spinal Cord Injury: Understanding Location, Function, Recovery, and the Future of Regeneration
The Highway of the Nervous System

By Dr. David Traster, DC, MS, DACNB
Co-owner, The Neurologic Wellness Institute
Boca Raton • Chicago • Waukesha • Wood Dale
www.neurologicwellnessinstitute.com
The spinal cord is one of the most important structures in the human body. While the brain often receives most of the attention, the spinal cord serves as the primary communication highway between the brain and every organ, muscle, gland, and sensory receptor in the body. Every movement you make, every sensation you feel, and every autonomic process that keeps you alive depends on information traveling through this remarkable structure.
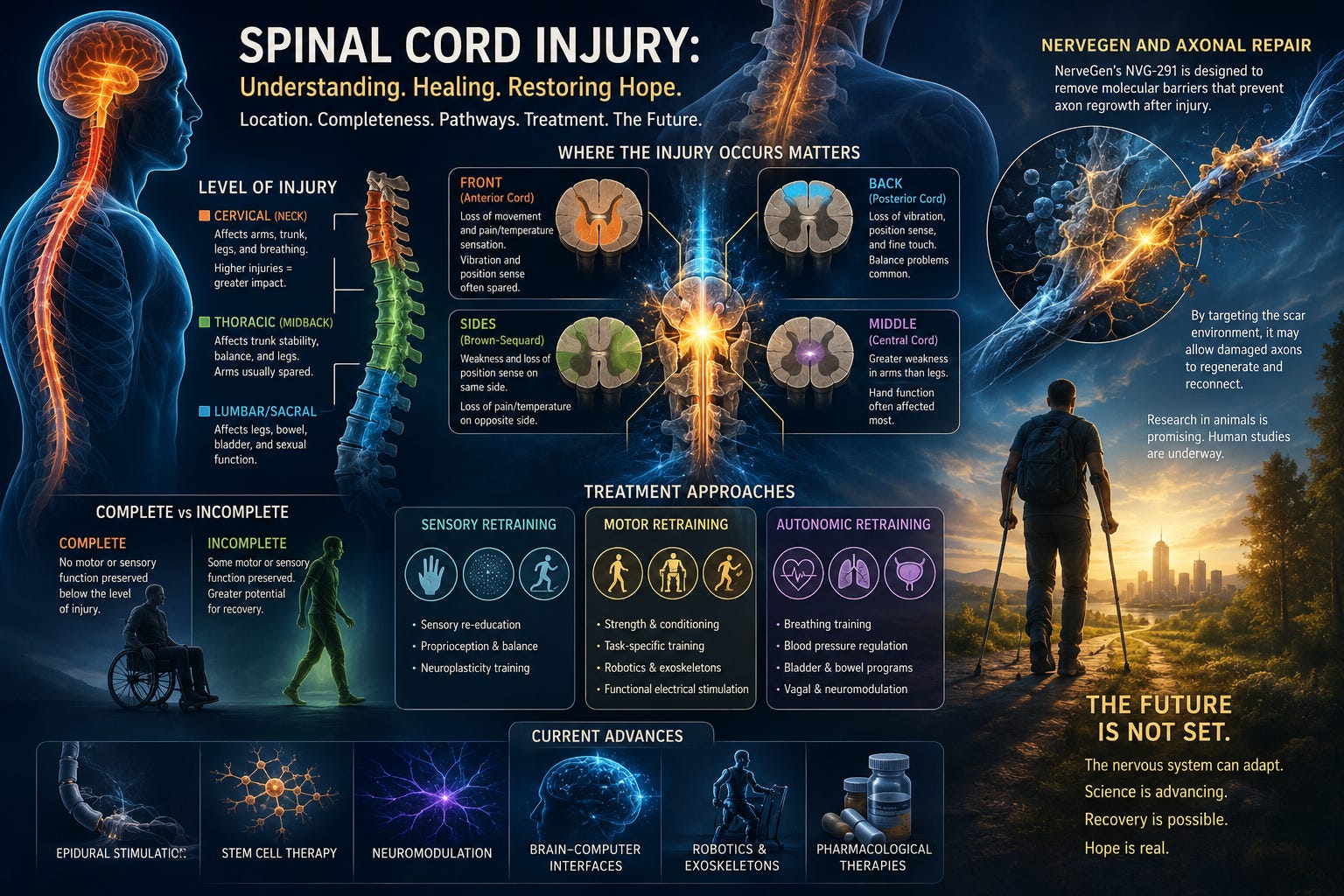
When the spinal cord is injured, communication between the brain and body becomes disrupted. The symptoms that develop depend on where the injury occurs, how much of the cord is damaged, and which specific pathways are affected. Understanding these principles helps explain why two people with spinal cord injuries may have dramatically different symptoms and recovery potential.
A Brief History of Spinal Cord Injury
For much of human history, spinal cord injury was considered a devastating and irreversible condition. Ancient Egyptian medical texts described spinal cord injuries as ailments “not to be treated.” Until the twentieth century, most severe spinal cord injuries resulted in death due to infections, respiratory failure, or complications related to immobility.
Advances in emergency medicine, surgery, rehabilitation, and intensive care dramatically improved survival rates. Today, many individuals live decades after spinal cord injury. More recently, advances in neuroplasticity, electrical stimulation, stem cell research, regenerative medicine, and axonal repair have begun to challenge the long-standing belief that recovery is impossible after spinal cord damage.
Complete Versus Incomplete Spinal Cord Injuries
One of the most important distinctions in spinal cord injury is whether the injury is complete or incomplete. A complete spinal cord injury means there is no preserved motor or sensory function below the level of injury. Communication between the brain and body is essentially interrupted across the entire width of the spinal cord.
An incomplete spinal cord injury means some pathways remain intact. Individuals may retain varying degrees of sensation, movement, autonomic function, or combinations of all three. Even very small amounts of preserved neural tissue can provide a foundation for neuroplasticity and functional recovery. Incomplete injuries generally have a more favorable prognosis because surviving pathways may strengthen, reorganize, and develop new functional connections over time.
Injuries of the Cervical Spinal Cord
The cervical spinal cord is located in the neck and contains pathways controlling the arms, trunk, legs, breathing muscles, and autonomic nervous system. Injuries at higher cervical levels often produce quadriplegia or tetraplegia, involving weakness or paralysis of all four limbs. Depending on the exact level of injury, individuals may experience respiratory compromise due to weakness of the diaphragm and accessory breathing muscles.
High cervical injuries can also affect blood pressure regulation, heart rate control, temperature regulation, bladder function, bowel function, sexual function, and sweating patterns. Because so much of the nervous system passes through the cervical cord, injuries here generally produce the most widespread deficits.
Injuries of the Thoracic Spinal Cord
Thoracic spinal cord injuries occur in the mid-back region. Because the arm pathways have already exited the spinal cord above this level, arm function is typically preserved. However, trunk control, abdominal function, balance, posture, autonomic regulation, and lower extremity function may be significantly impaired.
Individuals with thoracic injuries often experience paraplegia involving both legs while maintaining normal arm strength. Thoracic injuries can significantly impact respiratory mechanics because many of the muscles involved in forceful breathing originate from thoracic spinal segments.
Injuries of the Lumbar and Sacral Spinal Cord
Lumbar and sacral injuries affect the lower back region and the pathways controlling the legs, bladder, bowel, and sexual function. These injuries may produce weakness, sensory loss, gait abnormalities, foot drop, impaired balance, and changes in pelvic organ control.
Because many arm and trunk pathways remain intact, individuals with lumbar injuries often maintain greater overall independence than those with higher-level injuries. The exact pattern depends on whether the injury affects the spinal cord itself, the nerve roots, or the cauda equina.
Front of the Cord: Anterior Cord Syndrome
The front portion of the spinal cord contains many motor pathways as well as pain and temperature pathways. Individuals with anterior cord injuries often lose voluntary movement below the lesion and may lose pain and temperature sensation. However, vibration sense, proprioception, and joint position sense are often relatively preserved because these functions travel through the posterior columns located in the back of the cord. Anterior cord syndrome frequently results from vascular compromise involving the anterior spinal artery.
Back of the Cord: Posterior Cord Syndrome
The posterior spinal cord contains the dorsal columns, which carry vibration, proprioception, and position sense. Injuries here may produce severe sensory ataxia. Patients often feel unstable, uncoordinated, and unable to determine where their limbs are located in space. Walking becomes especially difficult in darkness because visual compensation is removed. Motor strength may remain relatively preserved despite profound balance dysfunction.
Side of the Cord: Brown-Sequard Syndrome
When one side of the spinal cord is injured, a characteristic pattern known as Brown-Sequard syndrome can occur. The individual typically develops weakness and loss of proprioception on the same side as the injury while experiencing loss of pain and temperature sensation on the opposite side. This occurs because different pathways cross the midline at different levels within the nervous system. Brown-Sequard syndrome provides one of the clearest examples of how neuroanatomy predicts clinical symptoms.
Middle of the Cord: Central Cord Syndrome
Central cord syndrome commonly affects the center of the spinal cord. Because arm pathways are positioned more centrally than leg pathways, arm weakness is often greater than leg weakness. Patients frequently have difficulty with hand dexterity, fine motor skills, buttoning clothes, writing, and manipulating objects. This syndrome is often seen after cervical hyperextension injuries.
Sensory Pathways, Motor Pathways, and Autonomic Pathways
The spinal cord is not a single structure performing one function. It contains sensory pathways carrying information toward the brain, motor pathways carrying commands away from the brain, and autonomic pathways regulating internal organs. Effective rehabilitation requires understanding which systems have been injured.
A patient with primarily sensory loss requires a different treatment approach than someone with motor weakness. Likewise, a patient with severe autonomic dysfunction may require targeted interventions focused on cardiovascular regulation, bladder function, temperature regulation, and autonomic stability.
Motor Rehabilitation
Motor rehabilitation focuses on strengthening surviving neural networks and promoting neuroplasticity.
Common approaches include:
Task-specific training
Body-weight supported treadmill training
Robotic gait training
Functional electrical stimulation
Strength training
Repetitive movement practice
Locomotor training
Exoskeleton-assisted walking
The nervous system learns through repetition. Thousands of repetitions create opportunities for surviving neural networks to strengthen and reorganize.
Sensory Rehabilitation
Sensory rehabilitation is often underappreciated despite its importance. The brain requires sensory input to construct movement accurately.
Treatment approaches may include:
Proprioceptive stimulation
Vibration therapy
Texture discrimination training
Sensory re-education
Visual-somatosensory integration
Balance training
Virtual reality environments
Sensory weighting exercises
Improving sensory processing can often improve motor performance indirectly.
Autonomic Rehabilitation
The autonomic nervous system is frequently affected after spinal cord injury.
Symptoms may include:
Orthostatic hypotension
Blood pressure instability
Heart rate abnormalities
Temperature dysregulation
Impaired sweating
Bladder dysfunction
Bowel dysfunction
Sexual dysfunction
Treatment strategies may include:
Tilt training
Respiratory rehabilitation
Vagal stimulation
Cardiovascular conditioning
Compression garments
Electrical stimulation
Biofeedback
Neuromodulation
Autonomic rehabilitation remains one of the most rapidly expanding areas of spinal cord injury care.
Electrical Stimulation and Neuromodulation
One of the most exciting developments in spinal cord injury rehabilitation involves spinal cord stimulation. Researchers have demonstrated that epidural stimulation can reactivate dormant neural networks below the injury.
Some individuals previously considered permanently paralyzed have regained standing, stepping, and voluntary movement after stimulation combined with intensive rehabilitation. These findings suggest that many spinal circuits remain viable but inaccessible without appropriate neuromodulatory input.
Stem Cells and Regenerative Medicine
Stem cell research seeks to replace damaged cells, support regeneration, reduce inflammation, and create a more favorable healing environment. Numerous clinical trials are underway exploring different stem cell types and delivery methods. While results remain variable, regenerative medicine continues to represent a promising avenue for future treatment.
Brain-Computer Interfaces
Another emerging technology involves brain-computer interfaces. These systems decode neural signals directly from the brain and use them to control external devices, robotic systems, or implanted stimulators. Recent studies have demonstrated individuals with paralysis controlling movement through direct brain-to-spinal-cord communication systems. These technologies may eventually bypass damaged spinal tissue entirely.
NerveGen and the Promise of Axonal Repair
One of the most closely watched developments in spinal cord injury research is the work of NerveGen. Following spinal cord injury, scar tissue develops around the damaged region. This scar contains molecules known as chondroitin sulfate proteoglycans that actively inhibit axonal regeneration.
NerveGen’s lead compound, NVG-291, is designed to overcome these inhibitory signals. Rather than replacing damaged neurons, the therapy attempts to remove molecular barriers that prevent surviving axons from reconnecting. Preclinical research has demonstrated improved axonal growth, enhanced functional recovery, and restoration of neurological function in multiple animal models.
Early human studies have focused primarily on safety and preliminary functional outcomes. While it remains too early to determine ultimate clinical effectiveness, the underlying biological mechanism is highly compelling and has generated significant excitement within the spinal cord injury community.
If successful, therapies such as NVG-291 may eventually be combined with rehabilitation, electrical stimulation, stem cells, and neuroplasticity-based interventions to create multidimensional treatment programs capable of producing far greater recovery than currently possible.
The Future of Spinal Cord Injury Recovery
The future of spinal cord injury treatment will likely not depend on a single breakthrough.
Instead, recovery may result from combining multiple strategies simultaneously:
Neuroplasticity-based rehabilitation
Electrical stimulation
Regenerative medicine
Stem cells
Brain-computer interfaces
Axonal repair therapies
Autonomic retraining
Advanced robotics
Pharmacological neurorestoration
For decades, spinal cord injury was viewed as a static condition. Modern neuroscience increasingly suggests that the nervous system remains capable of adaptation, remodeling, and recovery long after injury. While significant challenges remain, the field is entering an era where restoring function is becoming a realistic scientific goal rather than a distant dream. The story of spinal cord injury is gradually changing from one of permanent loss to one of possibility.
REFERENCES
Ahuja CS, Wilson JR, Nori S, Kotter MRN, Druschel C, Curt A, Fehlings MG. Traumatic spinal cord injury. Nature Reviews Disease Primers. 2017;3:17018.
Badhiwala JH, Wilson JR, Fehlings MG. Global burden of traumatic brain and spinal cord injury. The Lancet Neurology. 2019;18(1):24-25.
Kwon BK, Tetzlaff W, Grauer JN, Beiner J, Vaccaro AR. Pathophysiology and pharmacologic treatment of acute spinal cord injury. Spine Journal. 2004;4(4):451-464.
Fawcett JW, Curt A, Steeves JD, Coleman WP, Tuszynski MH, Lammertse D, Bartlett PF, Blight AR, Dietz V, Ditunno J, Dobkin BH, Havton LA, Ellaway PH, Fehlings MG, Privat A, Grossman R, Guest J, Kleitman N, Nakamura M, Gaviria M. Guidelines for the conduct of clinical trials for spinal cord injury. Spinal Cord. 2007;45(3):190-205.
Courtine G, Sofroniew MV. Spinal cord repair: Advances in biology and technology. Nature Medicine. 2019;25(6):898-908.
Angeli CA, Boakye M, Morton RA, Vogt J, Benton K, Chen Y, Ferreira CK, Harkema SJ. Recovery of over-ground walking after chronic motor complete spinal cord injury. New England Journal of Medicine. 2018;379(13):1244-1250.
Harkema S, Gerasimenko Y, Hodes J, Burdick J, Angeli C, Chen Y, Ferreira C, Willhite A, Rejc E, Grossman RG, Edgerton VR. Effect of epidural stimulation of the lumbosacral spinal cord on voluntary movement, standing, and assisted stepping after motor complete paraplegia. The Lancet. 2011;377(9781):1938-1947.
Rosenzweig ES, Brock JH, Lu P, Kumamaru H, Salegio EA, Kadoya K, Weber JL, Liang JJ, Moseanko R, Hawbecker S, Huie JR, Havton LA, Nout-Lomas YS, Ferguson AR, Beattie MS, Bresnahan JC, Tuszynski MH. Restorative effects of human neural stem cell grafts on spinal cord injury. Nature Medicine. 2018;24(4):484-490.
Bradbury EJ, Burnside ER. Moving beyond the glial scar for spinal cord repair. Nature Communications. 2019;10(1):3879.
Kucher K, Johns D, Maier D, Abel R, Badke A, Baron H, Thietje R, Casha S, Meindl R, Gomez-Mancilla B, Green BA. First-in-human phase 1 study of anti-Nogo-A antibody treatment in acute spinal cord injury. Neurology. 2018;91(9):e837-e847.