
Understanding Dysautonomia: Your Body’s Anti-Gravity System
The Autonomic Nervous System’s Fight to Keep Blood in the Brain

By Dr. David Traster, DC, MS, DACNB
Co-owner, The Neurologic Wellness Institute
Boca Raton • Chicago • Waukesha • Wood Dale
www.neurologicwellnessinstitute.com
Every time you stand up, your body faces a problem that physics guarantees—you should faint.
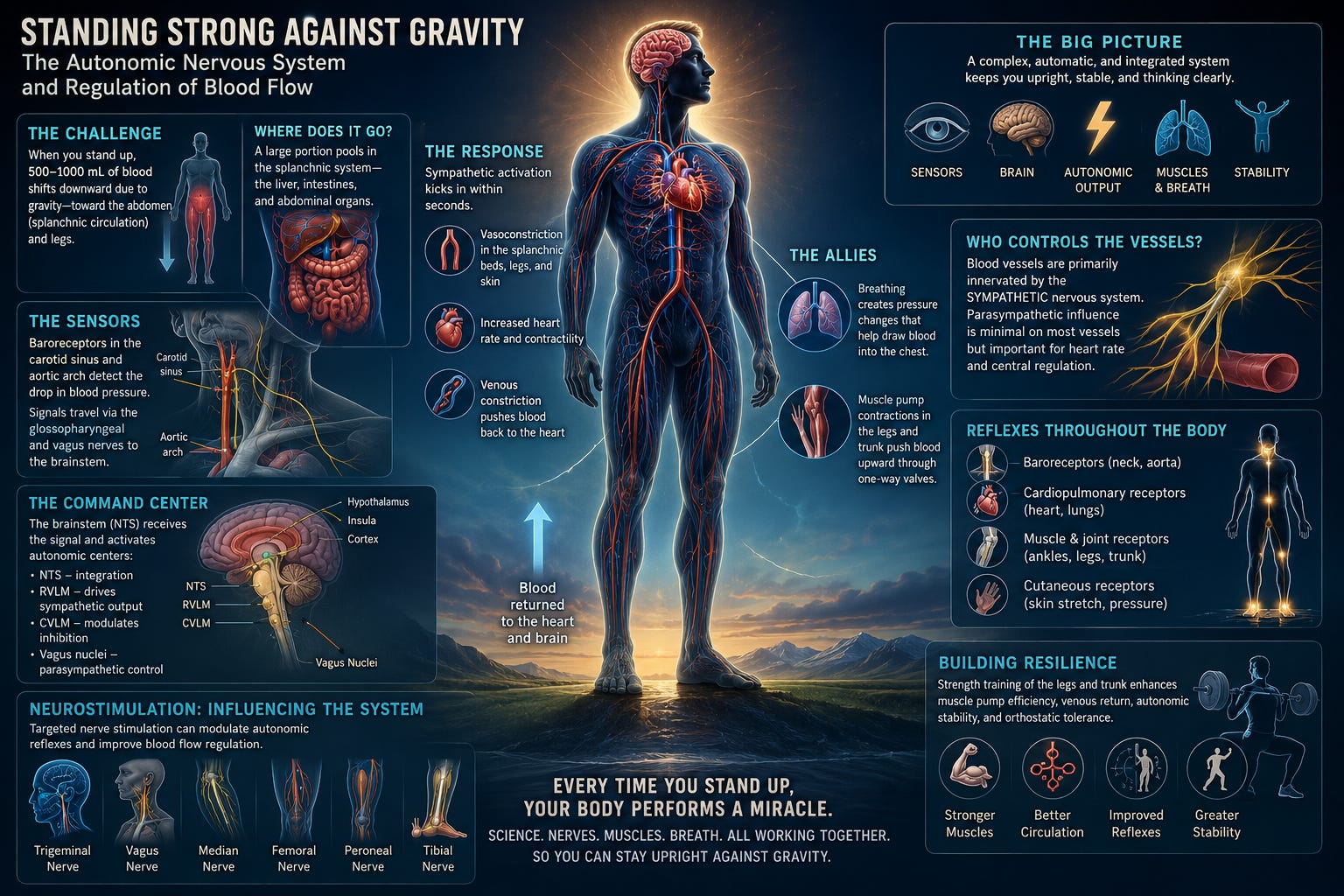
Gravity pulls blood downward, away from your brain, toward your abdomen and legs. Yet in a healthy system, you remain upright, clear-headed, and stable. This is not luck. It is the result of a highly coordinated, moment-to-moment orchestration between your autonomic nervous system, your muscles, your blood vessels, and your brain.
This system is so automatic that most people never notice it—until it stops working well.
The Immediate Challenge: What Happens When You Stand Up
The moment you move from lying or sitting to standing, approximately 500–1000 mL of blood rapidly shifts downward. A large portion of this volume pools within the splanchnic circulation—the blood vessels supplying the liver, intestines, and abdominal organs—which acts as a major reservoir.
At the same time, gravity pulls blood into the veins of the legs.
If unopposed, this would reduce venous return to the heart, decrease cardiac output, and drop blood pressure to the brain. Within seconds, you would experience dizziness—or lose consciousness entirely.
But the body intervenes immediately.
The Sensors: Detecting the Drop Before You Feel It
Your body relies on specialized pressure sensors called baroreceptors to detect changes in blood pressure.
The most important ones are located in:
The carotid sinus in the neck
The aortic arch near the heart
These receptors continuously monitor stretch in the arterial walls. When you stand and blood pressure briefly falls, the reduced stretch signals a problem.
This information is transmitted through cranial nerves:
The glossopharyngeal nerve (from the carotid sinus)
The vagus nerve (from the aortic arch)
These signals are sent to the brainstem, specifically to a region called the nucleus tractus solitarius (NTS).
The Brain’s Command Center: Rapid Autonomic Response
The NTS acts as the central processing hub. Within milliseconds, it coordinates a response involving:
The rostral ventrolateral medulla (RVLM) → drives sympathetic output
The caudal ventrolateral medulla (CVLM) → modulates inhibition
The dorsal motor nucleus of the vagus and nucleus ambiguus → parasympathetic control
Higher centers also contribute:
The hypothalamus integrates autonomic and hormonal responses
The insula and anterior cingulate cortex interpret internal body states
The cerebellum refines timing and coordination of cardiovascular responses
Together, these regions create a rapid shift toward sympathetic dominance.
The Effector System: How Blood Is Pushed Back to the Brain
Once activated, the sympathetic nervous system produces several key effects:
1. Vasoconstriction
Sympathetic fibers release norepinephrine onto alpha-1 receptors in blood vessels, causing them to constrict. This occurs especially in:
The splanchnic circulation
The legs and lower extremities
This reduces blood pooling and increases vascular resistance.
2. Increased Heart Rate and Contractility
Sympathetic stimulation increases:
Heart rate
Strength of contraction
This helps maintain cardiac output despite reduced venous return.
3. Venous Constriction
Veins constrict, pushing blood back toward the heart—critical for overcoming gravity.
The Muscle Pump: Your Second Heart
Your nervous system does not work alone.
The skeletal muscles of the legs and trunk act as a powerful mechanical pump. When they contract:
They compress veins
One-way valves prevent backflow
Blood is propelled upward toward the heart
This is why standing still for long periods can make you dizzy, while walking or shifting your weight prevents symptoms.
Strength and endurance of these muscles directly enhance your ability to tolerate gravity.
Breathing: The Overlooked Circulatory Engine
Breathing plays a major role in blood flow regulation.
During inhalation:
The diaphragm descends
Intrathoracic pressure decreases
Blood is “drawn” into the chest
During exhalation:
Pressure increases
Blood is pushed forward through the heart
This creates a respiratory pump that assists venous return.
Slow, controlled breathing can enhance vagal tone and stabilize cardiovascular responses, while erratic breathing can destabilize them.
Who Innervates Blood Vessels?
Most blood vessels are primarily controlled by the sympathetic nervous system.
Sympathetic fibers regulate vasoconstriction and tone
Parasympathetic influence on most peripheral vessels is minimal
However, parasympathetic activity (especially via the vagus nerve) indirectly influences blood pressure through heart rate and central regulation.
The balance between these systems determines whether your body maintains stability—or becomes symptomatic.
Reflexes Throughout the Body: More Than Just Baroreceptors
While baroreceptors are central, they are not the only players.
Cervical Reflexes
Mechanoreceptors in the neck provide positional information about head orientation relative to the body, influencing autonomic output.
Arterial and Cardiopulmonary Receptors
Sensors in the heart and lungs detect volume and pressure changes, adjusting sympathetic tone accordingly.
Lower Limb Mechanoreceptors
Receptors in the ankles, feet, and muscles detect load and movement, feeding into spinal and supraspinal circuits that influence vascular tone.
These systems integrate continuously to fine-tune blood flow.
Neuromodulation: How Peripheral Nerve Stimulation Influences Autonomic Control
Targeted stimulation of peripheral nerves can influence autonomic reflexes in powerful ways:
Trigeminal Nerve
Stimulation can influence brainstem autonomic centers, impacting blood pressure regulation and cerebral blood flow.
Vagus Nerve
Directly modulates parasympathetic output, reducing heart rate and influencing baroreflex sensitivity.
Median Nerve
Can enhance sympathetic modulation through central integration pathways and has been studied in blood pressure regulation.
Femoral, Peroneal, and Tibial Nerves
Activation of these nerves:
Engages muscle pumps
Stimulates afferent input to the spinal cord and brainstem
Enhances reflexive vascular responses
These inputs essentially “remind” the brain how to regulate blood flow more effectively.
Strength Training: Building a More Resilient Circulatory System
Strength training of the legs and trunk is one of the most powerful tools for improving orthostatic tolerance.
It enhances:
Muscle pump efficiency
Venous return
Vascular responsiveness
Autonomic stability
Stronger muscles mean less blood pooling, better circulation, and reduced strain on the autonomic nervous system.
Over time, this reduces symptoms like dizziness, fatigue, and lightheadedness.
The Integrated System: A Constant Negotiation With Gravity
Your ability to stand upright without symptoms is not a simple reflex—it is a dynamic, multi-system process involving:
Sensory detection
Central processing
Autonomic output
Mechanical assistance from muscles and breathing
When even one part of this system becomes inefficient—whether due to deconditioning, neurological dysfunction, injury, or chronic illness—the entire system can struggle.
And when it struggles, you feel it.
Dizziness. Fatigue. Brain fog. Instability.
Rewiring the System
The good news is that this system is highly adaptable.
Through targeted stimulation, movement, breathing, and strength training, the brain and body can relearn how to regulate blood flow more efficiently.
This is the essence of neuroplasticity applied to the autonomic nervous system—not just surviving gravity, but mastering it.
Because every time you stand up, your body is performing a complex neurological feat.
And when it works, it feels effortless.
But when it doesn’t, it becomes the mystery worth solving.
References
Benarroch, E. E. (2008). The arterial baroreflex: Functional organization and involvement in neurologic disease. Neurology, 71(21), 1733–1738.
Convertino, V. A. (2014). Blood volume: Its adaptation to endurance training. Medicine and Science in Sports and Exercise, 26(11), 1338–1348.
Freeman, R., Wieling, W., Axelrod, F. B., Benditt, D. G., Benarroch, E., Biaggioni, I., Cheshire, W. P., Chelimsky, T., Cortelli, P., Gibbons, C. H., Goldstein, D. S., Hainsworth, R., Hilz, M. J., Jacob, G., Kaufmann, H., Jordan, J., Lipsitz, L. A., Levine, B. D., Low, P. A., Mathias, C., Raj, S. R., Robertson, D., Sandroni, P., Schatz, I., Schondorf, R., Stewart, J. M., van Dijk, J. G., & Consensus Statement Group. (2011). Consensus statement on the definition of orthostatic hypotension. Clinical Autonomic Research, 21(2), 69–72.
Guyton, A. C., & Hall, J. E. (2021). Textbook of medical physiology (14th ed.). Elsevier.
Hainsworth, R. (2004). Pathophysiology of syncope. Clinical Autonomic Research, 14(Suppl 1), 18–24.
Kaufmann, H., Norcliffe-Kaufmann, L., & Palma, J. A. (2020). Baroreflex dysfunction. New England Journal of Medicine, 382(2), 163–178.
Rowell, L. B. (1993). Human cardiovascular control. Oxford University Press.
Thrasher, T. N. (2005). Baroreceptors and the long-term control of blood pressure. Experimental Physiology, 90(4), 347–352.
Victor, R. G., & Mark, A. L. (1985). Interaction of cardiopulmonary and carotid baroreflex control of vascular resistance in humans. Journal of Clinical Investigation, 76(4), 1595–1603.
Wieling, W., van Dijk, N., Thijs, R. D., de Lange, F. J., Krediet, C. T., & Halliwill, J. R. (2015). Physical countermeasures to increase orthostatic tolerance. Journal of Internal Medicine, 277(1), 69–82.