
The Gravity Map Inside Your Brain: The Neuroscience of Balance and Orientation
How vestibular, visual, and proprioceptive systems construct your sense of stability

By Dr. David Traster, DC, MS, DACNB
Co-owner, The Neurologic Wellness Institute
Boca Raton • Chicago • Waukesha • Wood Dale
www.neurologicwellnessinstitute.com
There is a force acting on you every moment of your life that you cannot see, cannot turn off, and cannot escape. It is constant, predictable, and silent—and your brain is working continuously to interpret it. That force is gravity. While we tend to think of gravity as a simple physical concept, within the nervous system it functions as a foundational reference point. It shapes how you stand, move, see, and even how safe you feel in your own body. When the brain accurately interprets gravity, everything feels stable and effortless. But when that interpretation becomes distorted, even slightly, the result can be dizziness, imbalance, muscle tension, and a persistent sense that something is “off.”
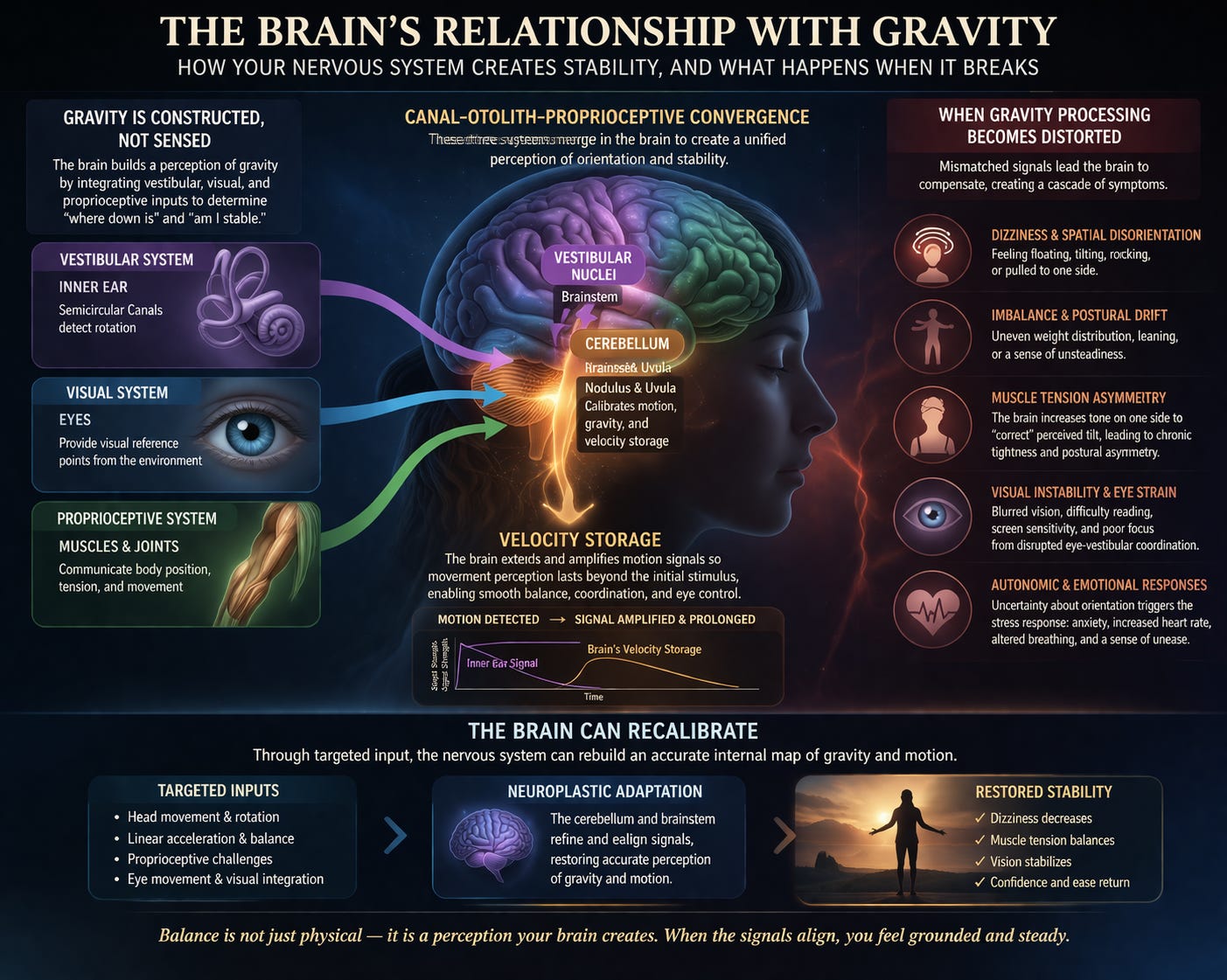
Gravity Is Constructed, Not Sensed
The body does not have a single receptor dedicated to detecting gravity. Instead, the brain constructs a perception of gravity by integrating multiple sensory systems. The vestibular system in the inner ear detects head movement and orientation in space. The visual system provides external reference points, helping you understand your relationship to the environment. The proprioceptive system, made up of signals from muscles and joints, informs the brain about body position and tension. These inputs are continuously sent to the brainstem and cerebellum, where they are combined into a unified perception of orientation. This process—multisensory integration—is essential for stability, and at its core lies canal–otolith–proprioceptive convergence. The semicircular canals detect rotational movement, the otolith organs detect linear acceleration and gravitational pull, and proprioceptors provide feedback about the body’s position. Together, they allow the brain to answer a simple but critical question: “Where am I relative to gravity?”
Velocity Storage and the Persistence of Motion
An important and often overlooked component of this system is velocity storage. The semicircular canals detect rotational movement, but their signals decay quickly. To compensate, the brain extends and amplifies these signals, allowing motion perception to persist longer than the initial sensory input. This process improves coordination, stabilizes vision through the vestibulo-ocular reflex, and enhances balance during sustained movement. However, when velocity storage becomes dysregulated, the brain may continue to perceive motion even after it has stopped. This can lead to symptoms such as lingering dizziness, motion sensitivity, delayed recovery after head movements, and discomfort in visually complex environments. These patterns are frequently observed in conditions like persistent postural perceptual dizziness, vestibular migraine, and post-concussion syndromes.
When Gravity Processing Becomes Distorted
When the brain struggles to accurately integrate gravitational and motion-related inputs, it begins to compensate. These compensations often manifest as dizziness and spatial disorientation. Individuals may feel as though they are floating, tilting, or being pulled to one side, even when they are physically stable. This is not due to actual movement, but rather a mismatch between sensory inputs and the brain’s internal model of orientation. Closely related to this is imbalance. Because posture is organized around gravity, any distortion in gravitational perception can lead to uneven weight distribution, postural drift, and an increased reliance on conscious effort to maintain stability. Many individuals describe a persistent feeling of leaning or unsteadiness, despite appearing normal on the outside.
Muscle Tension and Postural Asymmetry
One of the most overlooked consequences of disrupted gravity perception is asymmetrical muscle tension. When the brain perceives that the body is tilted or misaligned, it attempts to correct this by increasing muscle tone on one side. Over time, this leads to chronic tightness, particularly in the neck, shoulders, and hips, as well as broader postural asymmetries. These changes are not simply mechanical; they are neurologically driven responses to altered sensory input. The body is adapting to what the brain believes to be true, even if that perception is inaccurate.
Visual Instability and Eye Movement Dysfunction
The visual system is deeply dependent on stable vestibular input. When gravity and motion signals are inconsistent, the coordination between the eyes and the vestibular system becomes disrupted. This can result in drifting eye movements, poor convergence, and difficulty maintaining visual focus. Individuals may experience blurred vision, eye strain, difficulty reading, and increased sensitivity to screens or busy environments. These symptoms often appear to be purely visual but are frequently rooted in vestibular and cerebellar dysfunction.
Autonomic Responses and the Sense of Safety
The brain’s interpretation of gravity is also closely tied to the autonomic nervous system. Orientation in space is a fundamental component of how the brain determines safety. When the brain cannot confidently establish where the body is relative to gravity, it may interpret this uncertainty as a threat. This can activate the autonomic nervous system, leading to symptoms such as anxiety, changes in heart rate, altered breathing patterns, and a persistent sense of unease. These responses are not purely psychological—they are physiological reactions to a disrupted internal sense of stability.
The Role of the Cerebellum in Calibration
At the center of gravity perception and motion integration is the cerebellum, particularly regions such as the nodulus and uvula. These structures are responsible for calibrating sensory input, regulating velocity storage, and ensuring that vestibular, visual, and proprioceptive signals are aligned. When the cerebellum functions effectively, motion feels accurate, posture is stable, and the world appears steady. When it becomes dysregulated, sensory signals become mismatched, leading to the wide range of symptoms associated with dizziness and imbalance.
Recalibration Through Neuroplasticity
The most important implication of this system is that it is adaptable. These symptoms do not indicate that the brain is damaged beyond repair; rather, they reflect a miscalibrated system. Through targeted sensory input and training, the brain can relearn how to accurately interpret gravity and motion. Approaches such as vestibular rehabilitation and neuroplasticity-based therapies aim to restore proper integration by systematically stimulating the vestibular system, refining proprioceptive feedback, and improving visual coordination. Over time, this allows the brain to update its internal model of orientation.
Stability Is Something the Brain Creates
Balance is often thought of as a physical ability, but it is fundamentally a perceptual process. It is something the brain constructs from incoming sensory information and predictive modeling. When these inputs are aligned, you feel stable, grounded, and in control. When they are not, the world can feel uncertain and disorienting. The encouraging reality is that the brain has the capacity to recalibrate. With the right inputs and consistent exposure, it can rebuild its understanding of gravity, restore stability, and allow the body to move and function with ease once again.
References
Angelaki DE, Cullen KE. Vestibular system: The many facets of a multimodal sense. Annu Rev Neurosci. 2008;31:125–150.
Goldberg JM, Wilson VJ, Cullen KE, et al. The Vestibular System: A Sixth Sense. New York, NY: Oxford University Press; 2012.
Laurens J, Angelaki DE. The functional significance of velocity storage and its dependence on gravity. Exp Brain Res. 2011;210(3-4):407–422.
Raphan T, Cohen B. The vestibulo-ocular reflex in three dimensions. Exp Brain Res. 2002;145(1):1–27.
Cullen KE. The neural encoding of self-motion. Curr Opin Neurobiol. 2014;25:1–7.
Dieterich M, Brandt T. The bilateral central vestibular system: Its pathways, functions, and disorders. Ann N Y Acad Sci. 2015;1343:10–26.
Yates BJ, Bolton PS, Macefield VG. Vestibulo-sympathetic responses. Compr Physiol. 2014;4(2):851–887.
Borel L, Lopez C, Péruch P, Lacour M. Vestibular syndrome: A change in internal spatial representation. Neurophysiol Clin. 2008;38(6):375–389.
Straka H, Dieringer N. Basic organization principles of the VOR: Lessons from frogs. Prog Neurobiol. 2004;73(4):259–309.
Whitney SL, Herdman SJ. Physical therapy assessment of vestibular hypofunction. Neurol Clin. 2005;23(3):675–687.
Hola cómo estás hoy
Good article. With researching to understand myself better, I had wondered why I bump my shoulders into door frames amongst other things. I have a terrible time parking my car straight etc. I was diagnosed with ADHD a few years ago and the overlapping issue of navigation makes sense. I had correlated my muscle tension to just anxiety but now see another layer to this within your article. If you could respond with information related to my comment, I would appreciate it.